"You won’t see World War II veterans with these injuries. You won’t really see Korea or Vietnam veterans with these injuries,” says Gregory Galeazzi. “Plenty of them got them; they just didn’t survive them. Even though medicine has advanced, the majority of people who get these injuries still die on the battlefield.”
“But for a select few,” he adds, “they’re able to piece us back together. They send us out to be socially active and return to the workforce.”
Galeazzi, MD 2021, was a captain in the U.S. Army when he became one of the select few. During a routine patrol in Afghanistan’s Kandahar Province in May 2011, a roadside bomb blew off both his legs and nearly severed his right arm at the shoulder. Without the swift action of his fellow soldiers, who applied tourniquets and rushed their semiconscious platoon leader into a medevac, Galeazzi would have perished.
Instead, after more than fifty surgeries and hundreds of hours of physical therapy, Galeazzi is completing his first year as a medical student at HMS.
The estimated 1,800 U.S. military amputees returning home from recent conflicts in Iraq and Afghanistan have been injured to an extent rarely seen before. Although the technical sophistication of prostheses has grown over the centuries, artificial limbs have yet to attain the capabilities of natural ones. To support work toward that goal, the Department of Veterans Affairs and the Department of Defense fund the lion’s share of prosthetics research in the United States.
While Galeazzi attends class and clinic, scientists and clinicians throughout the HMS community are furthering the national effort by engineering prosthetic arms and legs that behave more like natural ones, pioneering brain-machine interfaces that create more intuitive connections between the nervous system and the prosthesis, and developing surgical techniques that allow for unprecedented prosthesis control and sensory feedback. Their work could benefit not only veterans but the other 98 percent of the two million people in the United States with limb loss due to diabetes, congenital conditions, cancer, and trauma, including accidents.
Perspective Shift
As innovations move from investigational stages to approval by the U.S. Food and Drug Administration, the broadening menu of options for amputees is changing millennia of clinical thinking.
“Historically, amputation has been viewed in the medical realm as a failure,” says Matthew Carty, an HMS associate professor of surgery at Brigham and Women’s Hospital, who is pushing the frontiers of amputation techniques and limb transplantation. “We need to talk about it as a reconstructive procedure and even a form of limb salvage. Physicians and patients need to consider the fact that amputation may be a faster and more effective pathway to better function and better life.”
“The biggest change I’ve seen in recent years is the societal understanding that losing a limb is not the end,” says David Crandell, an HMS assistant professor of physical medicine and rehabilitation at Spaulding Rehabilitation Hospital. Crandell managed the care of fifteen patients who underwent amputations following the 2013 Boston Marathon bombing. “People accept that technology can be part of the solution.”
In Search of the Natural
Because of his battlefield injuries, Galeazzi ended up with two transfemoral—above the knee, through the femur—amputations. Doctors salvaged his arm and fused the elbow. He worked up to wearing prosthetic legs for a few hours each day until a series of health setbacks and the demands of premedical studies derailed his progress. He lost so much bone density in his hips and spine that he fractured two vertebrae in a fall in early 2017. Now he uses a wheelchair, and he’s concerned that his reduced physical activity will affect his overall fitness.
“It took a ridiculous amount of energy to move those prostheses around,” he says. “I was sweating just going from the couch to the bathroom and back.”

Amputees confront dozens of potential health complications, from muscle atrophy and residual-limb infection, to low back pain and osteoarthritis from unnatural movement, to cardiovascular and metabolic disease from inactivity. Amputees who lose limbs in sudden events, losses known as traumatic amputations, often struggle with additional serious injuries, such as hearing damage, burns, and traumatic brain injury.
Developers of modern prostheses aim to alleviate some of these consequences and reduce pain by better mimicking the body’s natural biomechanics and improving walking efficiency. Experts estimate, for example, that walking with a traditional prosthesis takes about twice as much effort and is one-third slower than walking on two natural legs. Each step jars the body and dissipates energy by sending it into the ground rather than helping it rebound into the body. The advent of springy modern materials like carbon fiber started returning some of that energy to the wearer. Moreover, in the past fifteen years robotic components have begun to “restore a physiological pattern of motion,” says Paolo Bonato, an HMS associate professor of physical medicine and rehabilitation at Spaulding and director of the hospital’s Motion Analysis Laboratory.
One prothesis with robotic components, the PowerFoot BiOM, was created by Hugh Herr, PhD ’98, an HMS lecturer on physical medicine and rehabilitation at Spaulding and director of the MIT Media Lab’s Biomechatronics group. Bonato was involved in testing of it.
When an amputee steps down on this bionic prosthesis, springs that mimic tendons compress and store energy; when the wearer pushes off the ground, a battery-powered motor taps that stored energy and, like a muscle, propels the user forward with twice the energy of a natural leg. The device, which melds biology with technology, was the first to allow the prosthetic foot to flex in a physiological manner. It also incorporated microprocessors that adjust for speed and incline. Studies by Bonato and others indicate that the prosthesis, marketed as the Empower ankle, improves walkers’ balance, speed, and energy expenditure.
“Imagine you’re forced to walk around in clunky, stiff cowboy boots, and then suddenly you’re given lightweight Nikes and you can use your ankles again,” says Herr, who uses the BiOM. “It’s as distinct as going through the airport and hitting the moving walkway. It’s exhilarating.” Herr has been a world leader in bionic limb development since he lost both legs below the knee to frostbite in a 1982 mountain climbing trip.
Herr’s group continues to collaborate with Bonato’s to conduct complex analyses of human movement and energy expenditure, both to inform limb design and to gauge the success of those designs. Sometimes that means generating data on the intricate mechanics of a knee or studying muscle synergies in a reaching arm. More often, it involves measuring and modeling patient kinetics in the lab or sending patients home with wearable sensors to determine how well their prostheses work for them.
Not only will analyses inform the next generation of prosthetic limbs, but evidence of their health benefits could also expand access to them.
Restricted Movement
As medical director of the amputee care and adaptive sports programs at Spaulding, Crandell has seen his share of insurance denials for high-end prostheses. He chafes at some of the decisions on who deserves the best technology.
“Function and fairness are real societal issues,” he says.
When a computerized, battery-powered titanium leg can cost $75,000, only about 15 percent of amputees in the country, mainly those with amputations covered by VA or workers’ compensation policies, have a chance of having the cost covered. That group, however, is far outnumbered by the 54 percent of U.S. amputees who, according to the Amputee Coalition, have lost limbs to diabetes and other vascular diseases.
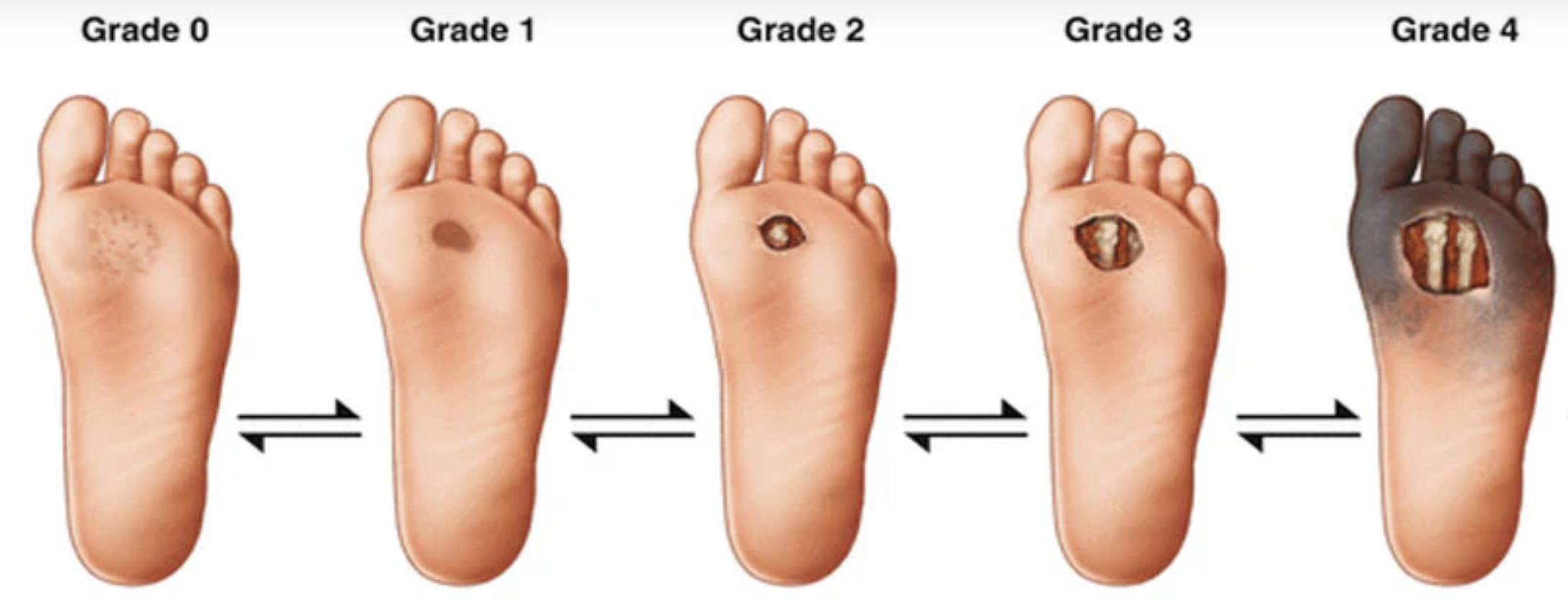
So far, people with diabetes who have had a lower-limb amputation, often older and in poor health, are not considered good candidates for advanced prostheses. Crandell and Bonato challenge this view. They’re experimenting with providing such patients with the best available technology, hoping that an easier-to-use prosthesis will encourage them to move more. If the program reduces complications such as second amputations, which occur in about 60 percent of people who lose one foot to diabetes, the researchers think insurance companies might reconsider their calculations.
Their hope may not be misplaced. Herr and colleagues nationwide recently got the U.S. Centers for Medicare & Medicaid Services to create a reimbursement code for bionic prostheses. The scientists plan to gather more data demonstrating improved gait and health to convince CMS to finalize coverage and pricing.
By Leaps and Bounds
Just before Darth Vader delivers shocking news to Luke about the Skywalker family tree in Star Wars: The Empire Strikes Back, he slices off Luke’s hand with a lightsaber. Vader’s revelation seems more traumatic for Luke than the loss of an extremity. It helps that he’s quickly fitted with a lifelike bionic prosthesis, one so sensitive it can detect the prick of a needle.

The scene made a lasting impression on Crandell, who first saw the movie while in high school. The future the scene depicted may, in fact, be near. “I can’t prescribe it yet, but I think the capacity for sensory feedback will exist in upper-limb prostheses in the next five years,” Crandell says.
Although upper-limb prostheses have had their breakthroughs in the past half-century, they largely haven’t progressed beyond hook hands. Amputees still give up on them at significantly higher rates than they do on legs. To close that gap, since 2008 DARPA has put more than $100 million into its Revolutionizing Prosthetics program for projects that focus on upper-limb development. That effort produced the DEKA Arm, renamed the LUKE Arm in honor of Skywalker. Approved by the FDA in 2014, the motor-powered above-elbow prosthesis has 10 degrees of freedom, six different hand grips, sensor-assisted feedback on grip strength, and the capacity to respond to wearer needs by moving multiple powered parts simultaneously rather than sequentially. Researchers are exploring new ways to control the DEKA Arm; HMS engineers are using it in brain–machine studies. A second arm being funded by DARPA uses electrodes implanted in both the brain and the residual limb to attempt neural control and sensory feedback.
At Spaulding, Bonato is collaborating with colleagues at Northeastern University on the development of a National Science Foundation-funded prosthetic hand controlled by a combination of muscle signals from the residual limb and electrical activity in the brain, as captured by electrodes embedded in a cap. The team is also adding cameras to prosthetic arms and using image-processing software to create prosthetic hands that anticipate what the wearer wants to do.
“If I’m approaching a button,” Bonato says. “I probably want to push it. You begin to narrow down the likely movements a person might want to perform.”
For legs as well as arms, the higher the amputation occurs on the limb, the harder it is to restore full function.
“Knees and elbows make all the difference in the world,” says Galeazzi.
A shorter residual limb has more prosthesis to haul around and fewer muscles and nerves with which to manipulate it. Multiple joints—elbow and wrist and fingers, or knee and ankle—must coordinate, and legs often need to coordinate with each other. The Herr lab is working on a power knee to join the Empower ankle as well as prosthetic leg enhancements that scan the terrain ahead and preemptively adjust power and angle.
"The blistering rate of miniaturization of cell phone and computer technology means engineers can pack a lot into the small space of a prosthesis."
“The blistering rate of miniaturization of cell phone and computer technology, with incredibly powerful microprocessor capabilities and accelerometers and so on, means engineers can pack a lot into the small space of a prosthesis,” says surgeon Carty.
Re-enabling basic activities may not be enough as amputees demand higher performance from their prostheses. Adults and children are 3-D printing limbs with custom features like water guns and vital-sign monitors. Kids are building and programming modules made of Legos to make their bionic hands perform different tasks. Typically young and fit, traumatic amputees itch to dive back into their active lives. The number of amputee soldiers able to requalify for active service rose from 2 percent in the 1980s to 16.5 percent by 2010, according to a study in The Journal of Trauma: Injury, Infection, and Critical Care.
“A lot of elderly amputation patients just want to walk between the bed and the toilet,” says Galeazzi. “We want to walk—and climb mountains, and snowboard, and run marathons, and surf. I’ve seen guys with the most advanced prostheses on the market come back after a weekend with the things snapped in half. They tell their prosthetists, ‘You have to do better.’”
Redirects
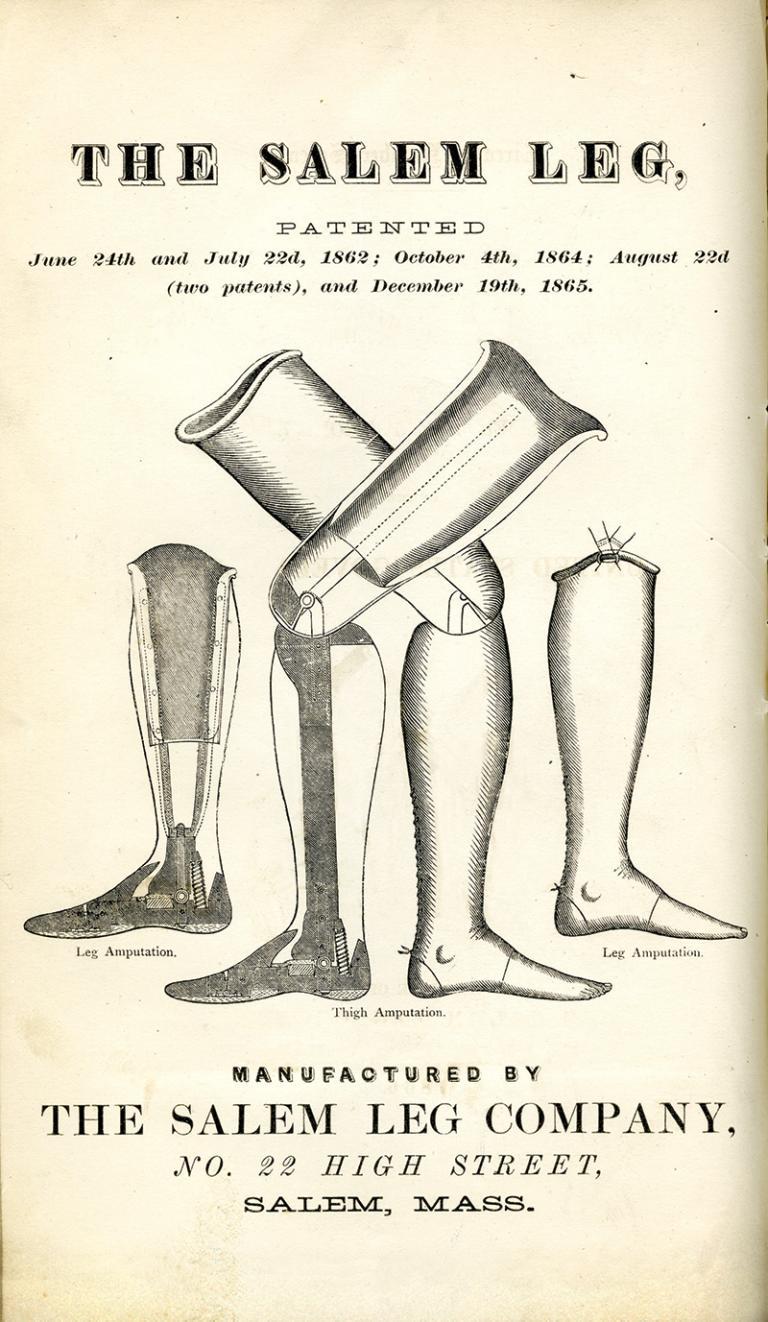
Although survival rates and prosthetic technologies have improved over the centuries, the surgical procedure for amputation has remained essentially the same.
"We see surgical manuals from the Civil War era and from a 2004 textbook and the surgical techniques are nearly identical."
“We see surgical manuals from the Civil War era and from a 2004 textbook and the surgical techniques are nearly identical,” says Shriya Srinivasan, a PhD candidate in the MIT-Harvard Program in Health Sciences and Technology, who is based in the Herr lab.
The standard technique of cutting a cross-section through the soft tissues before sawing off the bone means that severed nerves in the residual limb become unmoored, firing confused signals and often forming painful growths, while muscles that normally act in concert get disconnected. This shattering of physiology also prevents patients from taking full advantage of sophisticated prostheses.
“We haven’t asked much of the residual limb in the past,” says Carty. “Today’s technology demands more from it.”
Carty has joined forces with Srinivasan, Herr, and others to develop an alternative technique that preserves more of the limb’ s normal tissue relationships. They started with below-knee amputations. Carty takes tendons from the amputated ankle, anchors them to the residual tibia, and uses them to stitch together the ends of two muscles from the front and back of the leg so that when one contracts, the other stretches, as would occur in a normal leg.
The nerves that supply these muscles send clearer signals than those in traditional amputation and can receive basic signals in return. Implanted electrodes facilitate crosstalk between muscles, nerves, and prosthesis.
The researchers named the procedure AMI (pronounced “Amy”), for agonist-antagonist myoneural interface. They published a proof of concept in rats in 2017 and have now performed the operation on six human patients. What they’re seeing is promising. Patients have less pain and more natural function when using standard prostheses than do individuals with traditional amputations. Those who try advanced prostheses enjoy more intuitive control and greater range of motion. The procedure also restores a measure of proprioception, giving patients who wear a prosthesis a sense of its position without having to look. The team hopes it will also reduce phantom-limb pain.
Herr recalls the moment when the first AMI recipient attempted stairs in a lab test. The toe of his Empower ankle automatically pointed down to meet each step.
“We were shocked,” Herr says. “He could feel the prosthetic joint, and his brain and spinal cord knew what to do.”
Carty says the AMI technique may be able to be done as revision surgery in old amputations or in traumatic amputations. The main limitations are that it can’ t be performed on patients with nerve or vascular problems, such as diabetes. Because the procedure doesn’t involve any new or difficult surgical techniques, Carty is optimistic that it could be broadly adopted.
Carty and colleagues now have a proposal in IRB review to combine AMI with osseointegration, an experimental technique that attaches a titanium post directly to the bone in the residual limb. In place of the typical sleeve-and-socket attachment worn over the limb, the prosthesis latches onto a portion of the post that extends through the skin. The technique, devised by a pioneer of dental implants, Per-Ingvar Brånemark, has been undergoing tests with patients in Europe. In legs, osseointegration allows bone rather than soft tissue to bear the body’s weight and transmits a better feel for what’s underfoot. In arms and legs, the method could ease pain, reduce skin chafing and breakdown, and allow wearers to pursue activities that might cause a suction-adhered prosthesis to fall off. The main concern is risk of infection. The first U.S. trial to assess safety and feasibility began at the VA Salt Lake City Health Care System in 2015.
Mind Meld
Some HMS researchers seek to link prosthesis control directly with the brain.
Leigh Hochberg, an HMS senior lecturer on neurology, part-time, and director of the Center for Neurotechnology and Neurorecovery at Massachusetts General Hospital who also holds appointments at Brown University and the Providence VA Medical Center in Rhode Island, is principal investigator on an investigational brain-computer interface called BrainGate, a technology that aims to restore communication between the brain and either external devices or muscles in patients with conditions such as spinal-cord injury, brain-stem stroke, and amyotrophic lateral sclerosis.
To achieve the interface, a small electrode chip is implanted in the participant’s motor cortex, located at the “top” of the brain, to record the activity in a few dozen neurons. A small titanium pedestal attached to the skull conveys the neurons’ low-microvolt signals, which are then amplified and sent to a computer, where algorithms decipher the participant’s intention, for example, to move their hand “up and to the right.” The commands then get transmitted to a computer screen, a robotic or prosthetic arm not connected to the body, or to the participant’s own arm muscles via a separate muscle stimulation system.
The technology is exciting but still in its early days, Hochberg and others note. To capture all the data being transferred, the titanium pedestal is thus far physically connected to a computer. Although these trials are taking place in participants’ homes—exactly where, Hochberg says, clincially relevant technologies need to prove their utility—Hochberg and his BrainGate colleagues are actively working toward wireless implementation, a fully implantable version of the system, and improvements that would enable patients to use the system without research-team supervision.
Synthesis
Crandell sees more trainees each year who come into physical medicine and rehabilitation wanting to work with amputee populations. Interest also appears to be growing in other parts of the medical community. In addition to serving patient needs and driving new technologies, some are drawn to prosthetics development for the opportunity to collaborate with a range of specialists: mechanical, electrical, and tissue engineers; physicians and surgeons; neuroscientists, biologists, bioinformaticians, roboticists, nanotechnology specialists; prosthetists; and physical and occupational therapists.
While the bulk of projects are designed to improve devices and the way they interface with the body, others aim to reduce the need for prosthetic limbs. HMS surgeons have conducted successful single- and double-arm transplants. Carty now leads an effort to perform the nation’s first lower-limb transplant. Stem cell scientists are pursuing regenerative medicine to one day grow biological limbs.
Significant as those changes would be, people who have already had amputations don’t want to be left behind if they don’t want or do not qualify for advanced procedures, or if they represent too small a market for prosthetics development. “We don’t want to become the lost generation,” says Galeazzi.
The outlook among HMS researchers is optimistic for all amputees for at least two reasons. First, no single solution will be right for everyone.
“We have to ask what will give each patient the highest level of function and quality of life: multiple surgeries for limb salvage, a prosthesis, a transplant?” says Carty.
Second, some hold that biology isn’t necessarily better than synthetics.
“I’m not cellular- or tissue-centric,” says Herr. “Prostheses are part of the human story. It’s not something we’ll eliminate when we figure out how to do it with cells. In the future, we'll be hybrid.”
In many ways, we’re already hybrid. Prostheses—devices that support or replace body parts or functions—include not only limbs but hearing aids, cochlear implants, eyeglasses, dentures, pacemakers, and artificial knees and hips. Massachusetts Eye and Ear ophthalmologist Claes Henrik Dohlman developed an artificial cornea, the Boston Keratoprosthesis, in 1992. Neurosurgeon Shelley Fried at Massachusetts General Hospital and the Boston VA is designing retinal implants. An HMS team at Beth Israel Deaconess Medical Center pioneered 3-D printed molds for “airway prostheses,” stents that hold open patients’ tracheas. Last year, Harvard engineers built artificial muscles for soft robots. As much as half the human body can be replaced right now with artificial components.
For his part, Galeazzi wants the option of switching between a wheelchair and prosthetic legs; the first helps him travel long distances, the second would make it easier for him to navigate narrow exam rooms.
Although prostheses and alternatives have come far, there’s still ground to cover before every patient shares the sentiments of the amputee featured in “The One-Legged Man,” a 1916 poem by English poet Siegfried Sassoon. After losing a limb in the Great War, the poem’s narrator reflects in his elder years: “Thank God they had to amputate!”
Stephanie Dutchen is a science writer in the HMS Office of Communications and External Relations.
Images: iStock; courtesy of Ottobock (Empower ankle); John Soares (Carty and Srinivasan); Francis A. Countway Library/Boston Medical Library collection